A Response to the CY20 Opps Proposed Rule (CMS-1717-P)

A Response to the CY20 Opps Proposed Rule (CMS-1717-P) For Increased Price & Payment Disclosures
1) BACKGROUND
The CY20 OPPS Proposed Rule contains additional information and requirements regarding hospital price transparency. The proposal, which can be traced to guidelines provided in the Affordable Care Act, primarily follows several recent important government communications regarding this issue:
1) CURRENT DISCLOSURE REQUIREMENTS:
The FY19 IPPS Final Rule and subsequent responses to frequently asked questions:
a) The original FY19 IPPS Final Rule language, which reads:
“as one step to further improve the public accessibility of charge information, effective January
1, 2019, we announced the update to our guidelines to require hospitals to make available a list
of their current standard charges via the Internet in a machine readable format and to update
this information at least annually, or more often as appropriate. This could be in the form of the
chargemaster itself or another form of the hospital’s choice, as long as the information is in
machine readable format.”
b) The first responses to frequently asked questions posted at the end of September 2018
(https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/FAQs-Req-HospitalPublic-List-Standard-Charges.pdf)
c) A second responses to frequently asked questions posted in December 2018
(https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ProspMedicareFeeSvcPmtGen/Downloads/AdditionalFrequently-Asked-Questions-Regarding-Requirements-for-Hospitals-To-Make-Public-a-List-of-Their-Standard-Charges-via-theInternet.pdf)
2) PROPOSED DISCLOSURE REQUIREMENTS:
President Trump’s Executive Order on June 24, 2019 which was intended to provide patients access to pricing information for scheduled services and the out-of-pocket costs they may incur,
as well as to eliminate barriers to price and quality transparency, to increase the availability of meaningful price and quality information for patients and to enhance patients’ control over their own healthcare resources.
The order had three key dates for action and comment:
a. Within 60 days the Secretary of Health and Human Services would propose a regulation to require hospitals to publicly post standard charge information and negotiated rates for common or shoppable services in a consumer-friendly and machine-readable format
b. Within 90 days an advanced notice of proposed rulemaking would be made available for
comment on the proposal.
c. Within 180 days a report would be issued describing the manners in which the Federal Government or the private sector are impeding healthcare price and quality transparency for patients, and providing recommendations for eliminating these impediments in a way that promotes competition.
As a continuation of the FY19 IPPS Final Rule and to fulfill the requirement of President Trump’s Executive Order, the CY20 OPPS Proposed Rule has introduced additional clarification and requirements for hospitals. In the following pages, we will outline these key proposals with feedback to consider when responding in the comment window which ends on September 27, 2019.
2) CY20 OPPS PROPOSED RULE SUMMARY FOR ADDITIONAL CHARGE DISCLOSURE REQUIREMENTS
Nine areas pertain to the proposed requirements for hospitals to make public a list of their standard charges. Some of the areas represent further clarifications or definitions of terms outlined in the FY19 IPPS Final Rule and others are entirely new components. The nine areas are:
1) A definition of “hospital;”
2) Different reporting requirements that would apply to certain hospitals;
3) Definitions for two types of “standard charges” (specifically, gross charges and payer-specific negotiated charges) that hospitals would be required to make public;
4) A definition of hospital “items and services” that would include all items and services (including individual items and services and service packages) provided by the hospital to a patient in
connection with an inpatient admission or an outpatient department visit;
5) Requirements for making public a machine-readable file that contains a hospital’s gross charges and payer-specific negotiated charges for all items and services provided by the hospital;
6) Requirements for making public payer-specific negotiated charges for select hospital-provided items and services that are “shoppable” and that are displayed in a consumer-friendly manner;
7) Monitoring for hospital noncompliance with public disclosure requirements to make public standard
charges;
8) Actions that would address hospital noncompliance, which include issuing a written warning notice, requesting a corrective action plan, and imposing civil monetary penalties (CMPs) on noncompliant hospitals and publicizing these penalties on a CMS website; and
9) Appeals of CMPs.
We now summarize the key areas above with feedback to be considered by hospitals in their comments to the CMS.
3) A DEFINITION OF “HOSPITAL” & REPORTING REQUIREMENTS FOR DIFFERENT TYPES OF HOSPITALS
Summary: The transparency requirement in the FY19 IPPS Final Rule stated that “hospitals” needed to provide pricing information via the internet, but, did not define what organizations were “hospitals.” In the CY20 OPPS Proposed Rule, the CMS proposes to define a “hospital” very broadly to include most types of hospitals from all areas of the US and US territories. The only exceptions to the reporting requirements would be “Federally-owned or operated institutions (for example, hospitals operated by an Indian Health Program, the US Department of Veterans Affairs, or the US Defense Department)” as these facilities “are not accessible to the general public, except in emergency situations, and already make their charges publicly available are deemed to have met the requirements of Section 2718(e).” Ambulatory Surgical Centers (ASCs) or other non-hospital sites-of-care (lab, imaging centers) are also excluded.
Comment: After the FY19 IPPS Final Rule, there was some confusion of what constituted a hospital. A case could to be made that non-enrolled Medicare institutions as well as institutions not paid
prospectively could take issue with parts or all of the reporting requirements. As an example, those hospitals not paid prospectively via Medicare MSDRGs could take issue with having to report charges based on this grouping methodology. We would encourage hospitals that feel strongly that these reporting requirements should not apply to them for these reasons to comment along these lines.
4) A DEFINITION OF “STANDARD CHARGES” & “ITEMS AND SERVICES”
Summary: The CMS proposes defining standard charges as both GROSS charges, as well as “payerspecific negotiated charges.” Essentially, the latter refers to the payment rates that are agreed to by the hospital and the payer.
In addition, the CMS is defining what is meant by providing pricing information for “all items and services” to be inclusive of:
1) All items in the chargemaster and/or provided to patients, including drugs and supplies
2) Charges for “Service Packages” – meaning, all other types of “aggregation of individual items and services into a single service with a single charge” the hospital could be paid under – including, MSDRGs, per diems, and other packages including those in outpatient settings
3) Charges for employed physicians and non-physician practitioners
Comment: The combination of these definitions pose significant challenges for reporting and in many cases are not technically possible. While we understand the intent of each request, we believe additional information will be helpful in refining the requirements to something that will meet the spirit of the rule in a way that is also technically feasible for hospitals.
1) SERVICES: Chargemaster (CDM) information – gross charges reporting are entirely possible at the line level and are already a part of the FY19 IPPS rule disclosure requirements. However,
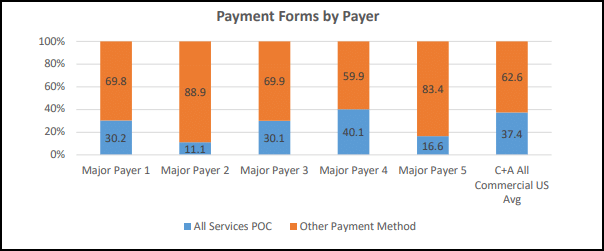
payer-specific negotiated charges cannot be reported for a majority of hospital contracts at the CDM line level. Our firm represents over 400 hospitals annually for pricing defensibility and
viability projects and in those projects, we model all hospital contracts and payment terms. We have found that less than 40% of payment terms are entirely percentage of charge (POC) based
where this type of payer-specific negotiated charge reporting would be possible at the CDM line level. And, that rate is highly variable depending on the payer. The table below provides a
distribution of the POC-based contracts for five of the most prevalent national payers, as well as our national all-commercial payment term average.
2) SERVICE PACKAGES: Item aggregations – we completely agree that aggregated information will be more useful to patients than CDM line information. We also agree, in part, with the CMS’
definition of service packages to be an “aggregation of individual items and services into a single service with a single charge.” However, some of the examples provided do not always represent a single charge (“common procedure” schedules and “per diems” commonly include additional carveouts, hierarchy rules, and multiple payment logic that prohibit “single charge” establishment). In addition, while hospitals have payer-specific negotiated rates for these service packages, they do not set GROSS charge rates for them. Gross charges are ONLY established at the CDM line level. All other gross charge reporting would need to be representative of averages. There is a more significant issue, though, with the current definition: these service packages will still not provide the patient with an understanding of their total charge responsibility because there would be a combination of service packages to equal their total gross charge for their entire encounter. That is why we believe the CMS is really trying to provide patients with an understanding of their total claim or encounter charge responsibility. In that way, the only STANDARDIZED and SINGLE payment per claim payment methodology is Medicare’s MSDRG system. Gross charge averages could be provided for all MSDRGs. In addition, because the Medicare grouping logic is publicly available, an AVERAGE payment across all payers could be provided. We would caution against payer-specific disclosure for three primary reasons:
a. Outlier cases and patient demographic variation could impact the averages significantly using this average as a complete basis for comparison could lead to faulty conclusions.
b. In most payer contracts, the payment terms/rates are proprietary and protected. Disclosing specific rates could lead to significant legal challenges and costs for local and national stakeholders. An average across all payers would permit an understanding of the gross to net reimbursement relationship for patients and would be far less likely to be challenged legally. Similarly, the disclosure of specific payment information would guard against anti-competitive behavior noted by the CMS.
c. Disclosing the entirety of this information would be highly burdensome for hospitals and ultimately is best suited to be provided by the payers through transparency tools they are creating to drive down member costs. Payers have the most current payment terms for all providers and can do the comparison evaluations for the patients – and – are incented to do so. Further, payers have the most up-to-date information on patient payment responsibility and can provide the most accurate estimates for proposed care.
3) EMPLOYED PHYSICIAN & NON-PHYSICIAN PRACTITIONER FEES: Employed physician and nonphysician practitioner fees should be excluded from the definition of all items and services for
three primary reasons:
a. Substantial variation exists among hospitals for the level of employment of professional services. This would present significant issues for the patient when they are trying to compare charges (there could be an assumption that a hospital without employed physicians will have lower charges) or trying to understand their charges for a service at a single hospital (certain specialties could be employed but others not, making disclosure and understanding highly challenging for the patient).
b. In many instances, the employment of physicians and non-physician practitioners represent complicated legal organizational structures where the hospital does not technically employ these professionals, but rather other separate legal entities.
c. Disclosure of payer-specific negotiated charges for these services also has a high degree of probability for legal challenge and anti-competitive behavior. We again believe the disclosure of payer-specific negotiated charges should be done by payers through member tools.
In summary, we present the table below to highlight what is possible for reporting under each proposed scenario:
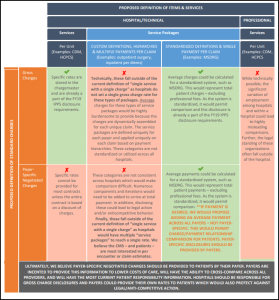
5) REQUIREMENTS FOR DISCLOSING STANDARD CHARGES FOR ALL ITEMS AND SERVICES IN A MACHINE READABLE FORMAT
Summary: The CMS is seeking uniformity in the way that hospitals post their standard charges and proposing that the disclosure include the following elements:
1) Description of each item or service (including both individual items and services and service
packages).
2) The corresponding gross charge that applies to each individual item or service when provided in,
as applicable, the hospital inpatient setting and outpatient department setting.
3) The corresponding payer-specific negotiated charge that applies to each item or service (including charges for both individual items and services as well as service packages) when provided in, as applicable, the hospital inpatient setting and outpatient department setting. Each list of payer-specific charges must be clearly associated with the name of the third-party payer.
4) Any code used by the hospital for purposes of accounting or billing for the item or service, including, but not limited to, the Current Procedural Terminology (CPT®) code, Healthcare
Common Procedure Coding System (HCPCS) code, Diagnosis-Related Group (DRG), National Drug Code (NDC), or other common payer identifier.
5) Revenue code, as applicable.
Other key reporting components include:
1) Machine readable formats: including, but not limited to, .XML, JSON and .CSV formats. A PDF would not meet the definition because the data contained within the PDF file cannot be easily
extracted without further processing or formatting.
2) Location: while the hospital has discretion of where to post the disclosure, it must be on a publicly-available webpage, displayed prominently and easily accessible, without barriers, but with the ability to be digitally searched.
3) Updates: at least annually and date of last update must be clearly labeled. Comment: It likely was only a matter of time for the CMS to include a HCPCS/CPT® value to the disclosure as it will permit the ability for comparison. Because of the variation among hospitals with price bundling and utilization differences, the importance of having a disclosure of average charges by encounter is likely more relevant than ever to help better communicate gross charge comparisons.
Comment: It likely was only a matter of time for the CMS to include a HCPCS/CPT® value to the disclosure as it will permit the ability for comparison. Because of the variation among hospitals with price bundling and utilization differences, the importance of having a disclosure of average charges by encounter is likely more relevant than ever to help better communicate gross charge comparisons.
6) REQUIREMENTS FOR CONSUMER-FRIENDLY DISPLAY OF PAYER-SPECIFIC CHARGES FOR SELECTED SHOPPABLE SERVICES
Summary: The CMS proposes to have an additional disclosure document that would be made available on the internet for patients to access payer-specific negotiated charges for a set of 300 services (70 identified by CMS and 230 at the discretion of the hospital) that are deemed to be shoppable. Shoppable is defined as a service package that can be scheduled by a patient in advance. In addition to the disclosure of the payer-specific negotiated charges for the specific service, all charges for ancillary services associated would need to be provided as well. Specifically, the CMS is proposing that the consumer-friendly display of payer-specific negotiated charge information contain the following corresponding information for each of the 70 CMS-selected and at least 230 hospital-selected shoppable services:
1) A plain-language description of each shoppable service.
2) The payer-specific negotiated charge that applies to each shoppable service. If the hospital does not provide one or more of the CMS-selected shoppable services, the hospital may indicate
“N/A” for the corresponding charge or otherwise make it clear that the service is not provided by the hospital. Each payer-specific charge must be clearly associated with the name of the third-party payer.
3) A list of all the associated ancillary items and services that the hospital provides with the shoppable service, including the payer-specific negotiated charge for each ancillary item or service.
4) The location at which each shoppable service is provided by the hospital (for example, Smithville Campus or XYZ Clinic), including whether the payer-specific negotiated charge for the shoppable service applies at that location to the provision of that shoppable service in the inpatient setting or the outpatient department setting or both. If the payer-specific negotiated charge for the shoppable service varies based upon location or whether the hospital provides the shoppable service in the inpatient setting versus the outpatient setting, the hospital would be required to
identify each payer-specific negotiated charge.
5) Any primary code used by the hospital for purposes of accounting or billing for the shoppable service, including, but not limited to, the Current Procedural Terminology (CPT®) code, the Healthcare Common Procedure Coding System (HCPCS) code, the Diagnosis-Related Group (DRG), or other commonly used service billing code.
Comment: We agree a separate disclosure of highly shoppable services could be more beneficial for consumers than the current disclosure requirements for the entire price list of all CDM items. However, we do not believe the current requirement will be technically possible for hospitals to provide for several key reasons:
1) Payer-specific negotiated charges do not exist for most – if not all – of the items currently on the list. Payment is at the claim level for patients and most of the items on the list are line/procedure level items. Unless the contract is completely percent of charge based, the hospital could not provide this information.
2) Gross charges are not established for a number of codes on the proposed list. As a primary example, surgical procedure codes typically do NOT have hardcoded lines and prices in the CDM. Instead, operating room prices (on a basis of charge per minute, as example) are utilized and HIM professionals later “soft code” the CPT® based on the utilization of time and the type of
procedure(s) performed on the patient.
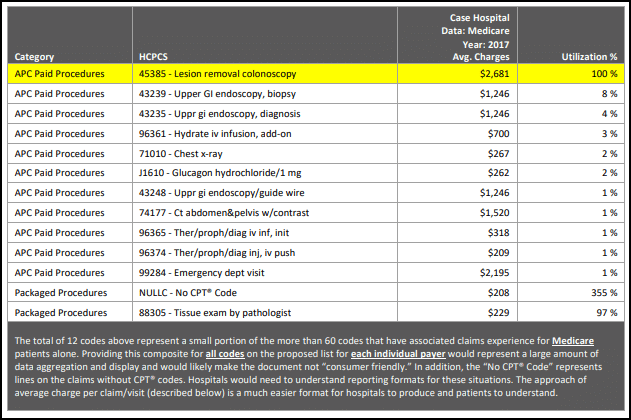
3) Associated ancillary service charges could be provided under the MSDRG system, but, not for most other payer payment structures as it would be highly variable. To highlight this, we provide
a case example hospital and the national hospital average for average GROSS charge and utilization per claim for associated items during an outpatient colonoscopy. The example is built using Medicare claims data and highlights several key challenges for reporting this information for the entire list of proposed codes for each individual payer:
a. In total, the case hospital had more than 60 codes for Medicare alone for this one CPT®example. Providing this for every code on the proposed list for every payer would be a significant administrative burden for hospitals and would not make the list consumer friendly.
b. The case hospital – and many in the US – do not have a hardcoded CDM price for CPT® 45385. To illustrate, we sampled 174 hospital CDMs from 2019 and found that only 36% have a hardcoded price for this CPT®.
c. Payment for the case hospital – and many in the US – can include multiple procedure payment rules (note that there can be multiple procedures performed) and provision of this information would be challenging and potentially highly misleading. Again, we believe payer negotiated charges should be provided by the payers.
d. At what point would a hospital not need to provide information on an associated code? 5% utilization, 1% utilization, ANY utilization? Note in the example below that the case hospital will include a CT of the abdomen & pelvis 1% of the time with a charge of $1,520. That could be an important element for patients to know, but, if rules are established on a “posting threshold” then these could be missed. And yet, if the threshold is set too low, a vast amount of data could need to be provided that would not make the disclosure consumer friendly.
HCPCS 45385 Associated Ancillary Charge Example Under Proposed Requirements
As a result of the above information, we would recommend the following be adopted for the consumer friendly disclosure:
1) MODIFY: 70 CMS selected and at least 230 hospital-selected shoppable services. MODIFY TO 70 CMS SELECTED AND AT LEAST 30 HOSPITAL-SELECTED SHOPPABLE SERVICES. This figure could be expanded in the future, however, we propose beginning with a smaller number to make the disclosure more manageable for patients.
2) MAINTAIN: A plain-language description of each shoppable service.
3) MODIFY/REMOVE: The payer-specific negotiated charge that applies to each shoppable service. If the hospital does not provide one or more of the CMS-selected shoppable services, the 9 A Response to CY20 OPPS Proposed Rule for Additional Price & Payment Disclosures hospital may indicate “N/A” for the corresponding charge or otherwise make it clear that the
service is not provided by the hospital. Each payer-specific charge must be clearly associated with the name of the third-party payer. MODIFY TO AVERAGE GROSS CHARGE DISCLOSURE ANDREMOVE PAYER-SPECIFIC CHARGES AS THESE DO NOT EXIST FOR MOST HOSPITALS AT THE CODE LEVEL FOR THE PROPOSED CODES.
4) MODIFY: A list of all the associated ancillary items and services that the hospital provides with the shoppable service, including the payer-specific negotiated charge for each ancillary item or
service. MODIFY TO AVERAGE CLAIM CHARGE FOR THE PRIMARY ITEM AND ALL ASSOCIATED ITEMS. THIS WILL PROVIDE THE NECESSARY INFORMATION FOR PATIENTS IN A MUCH EASIER SUMMARIZATION AND WOULD ELIMINATE THE ISSUES OF INCLUSION/EXCLUSION OF CERTAIN ITEMS WITH DIFFERING UTILIZATION PERCENTAGES.
PROPOSED CONSUMER FRIENDLY HCPCS 45385 Associated Ancillary Charge Example

5) MODIFY: The location at which each shoppable service is provided by the hospital (for example, Smithville Campus or XYZ Clinic), including whether the payer-specific negotiated charge for the
shoppable service applies at that location to the provision of that shoppable service in the inpatient setting or the outpatient department setting or both. If the payer-specific negotiated charge for the shoppable service varies based upon location or whether the hospital provides the shoppable service in the inpatient setting versus the outpatient setting, the hospital would be required to identify each payer-specific negotiated charge. MAKE THIS COMPONENT OPTIONAL FOR GROSS CHARGE REPORTING (REMOVE PAYER-SPECIFIC NEGOTIATED CHARGES.) THE HOSPITAL MAY NOT HAVE SEPARATE PRICING AND IF IT DOES AND THE PRICING IS LOWER IT WILL LIKELY WANT TO EMPHASIZE THIS FOR PATIENTS.
6) MAINTAIN: Any primary code used by the hospital for purposes of accounting or billing for the shoppable service, including, but not limited to, the Current Procedural Terminology (CPT®)
code, the Healthcare Common Procedure Coding System (HCPCS) code, the Diagnosis-Related Group (DRG), or other commonly used service billing code.
7) NONCOMPLIANCE
Summary: One final key point is that the CMS proposes a penalty of up to $300 per day for noncompliance. This would amount to $109,500 for a hospital that was not compliant for an entire year.
Comment: We understand that it was only a matter of time for the CMS to create penalties for noncompliance. We encourage hospitals that disagree with the proposed penalties to submit comments to the CMS within the feedback window ending September 27, 2019.
8) FINAL THOUGHTS
We certainly support reasonable efforts to continue to help patients understand the financial implications of their care. However, we believe that the amount of additional data being required is not always technically possible to post and could lead to a number of unintended consequences – including legal action and anti-competitive behavior. These elements could cause more patient confusion and potentially drive up the costs of healthcare which are counter to the spirit of the law. We hope that the additional comments provided will be considered in revising the proposed requirements to be technically possible as well as consumer friendly.
We do share some concern that much of this additional disclosure information will go unutilized by patients. The introductory narrative provided by the CMS in the Proposed Rule includes a defense for the promotion of additional transparency in healthcare and how that will lead to reduced costs. However, it is interesting to note that one of the referenced sources (Desai S, Hatfield LA, Hicks AL, et al. Association Between Availability of a Price Transparency Tool and Outpatient Spending. JAMA. 2016;315(17):1874-1881. Concludes the opposite, finding:
In this analysis, offering a health care services price transparency tool to employees was not associated with lower outpatient spending. This was also true in sub analyses focused on employees with higher health plan deductibles and those with comorbidities at baseline. Furthermore, those offered the price transparency tool did not shift their care from higher-priced HOPD settings to lower-priced ambulatory settings.
The same article also runs counter to other “benefits” the CMS believes will occur with increased reporting of the newly proposed requirements:
A series of factors may underlie the lack of a negative association between offering the price transparency tool and outpatient spending. First, despite selecting 2 employers with the highest uptake and substantial marketing from the employers, use of the tool was relatively low, with only 10% of employees logging on in the first year of its introduction. Such low use rates have been reported for other price transparency tools. Moreover, low utilization is the most commonly reported challenge to price transparency initiatives by insurers who offer tools. Patients may not find the information compelling or may simply forget about the tool if they seek health care infrequently.
Second, there may be limited opportunities for patients to save money via the tool. Price shopping is most useful for care that is nonemergent and of lower cost, and there may be a limited set of services that meet those criteria. A recent report found that only 40% of spending is attributable to shoppable services. In this study, a substantial fraction of searches were for services whose prices exceeded the employee’s deductible, so that out-of-pocket amounts would be the same regardless of which clinician or hospital was chosen. Also, approximately half of employees met their deductible within the year. After reaching their deductible, patients may have little incentive to price shop. Third, a common service through which patients could benefit from price shopping is clinician office visits. However, many patients have established relationships with their clinicians that they may wish to maintain regardless of price.
We hope that this information has been useful to summarize the numerous proposed disclosure requirements and provide some commentary on the challenges with many of the components.
Given these concerns, we highly encourage hospitals to submit feedback to the CMS within the comment window which ends on September 27, 2019 at 5pm EDT.
RESPONDING TO THE CMS
The following information provides direction from the IPPS proposed rule for commenting:
DATES: Comment Period: To be assured consideration, comments on this proposed rule must be received at one of the addresses provided in the ADDRESSES section no later than 5 p.m. EST on
September 27, 2019.
ADDRESSES: In commenting, please refer to file code CMS-1717-P. Because of staff and resource limitations, we cannot accept comments by facsimile (FAX) transmission. Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
1) Electronically. You may submit electronic comments on this regulation to http://www.regulations.gov. Follow the “Submit a comment” instructions.
**Search for CMS-1717-P and select “Comment Now” from search results
2) By regular mail. You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1717-P,
P.O. Box 8013, Baltimore, MD 21244-1850. Please allow sufficient time for mailed comments to be received before the close of the comment period.
3) By express or overnight mail. You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1717-P, Mail Stop C4-26-05,7500 Security Boulevard, Baltimore, MD 21244-1850.
To download this PDF click here and to access the rest of our Hospital Research PDFs click here.
Have thoughts or questions?
Related