Are Patient Rights Advocate’s Compliance Reports Accurate?
Patient Rights Advocate Dramatically Overstates Hospital Non-compliance
Last month, PatientRightsAdvocate.org (PRA) released its Sixth Semi-Annual Hospital Price Transparency Compliance Report (https://www.patientrightsadvocate.org/semi-annual-report-feb2024). The report shows that 34.5% of the 2,000 US hospitals it reviewed comply with federal price transparency requirements. Unfortunately, PRA’s findings continue to be horribly flawed. HFMA, AHA, and even CMS have countered the findings in different statements and reports over the past year:
- CMS Findings that 70% of US hospitals are fully compliant
- AHA Statement on PRA
- HFMA Statement on PRA
As we have done previously, we will highlight where PRA is insufficient in its knowledge and application of the federal transparency requirements within its research and findings.
PRA Findings
▪ PRA Findings: 65.1% of the hospitals (1,303/2,000) did not post a complete machine-readable file of standard charges. 48.6% of the hospitals (972/2,000) did not publish a sufficient amount of negotiated rates.
PRA defined “complete” and “sufficient” as meeting the following criteria:
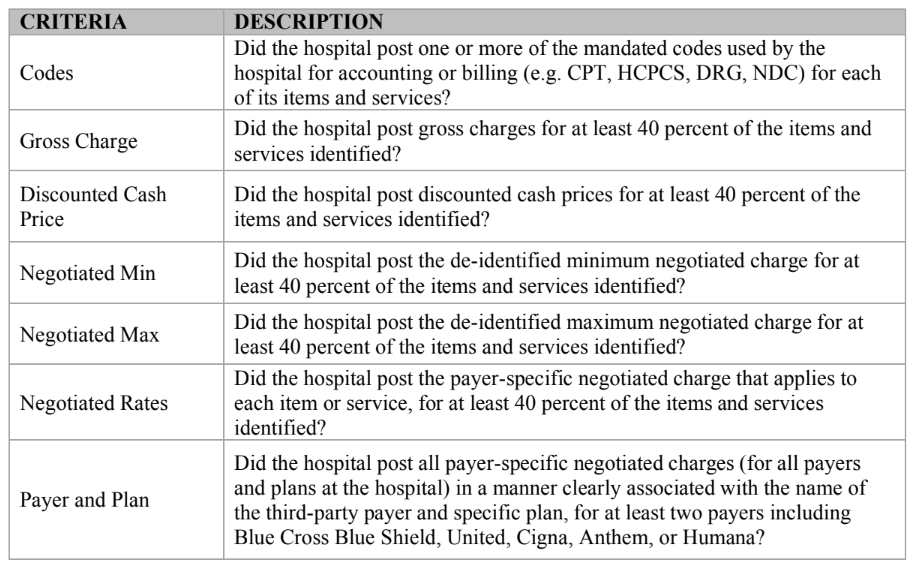
PRA says that a hospital was found NONCOMPLIANT in their report if there was a “no” response for any of the above criteria. However, PRA’s criteria clearly show its lack of knowledge of the federal price transparency requirements and a hospital’s billing environment. For example, for many of the fields, PRA has established a threshold of “40 percent” populated values in order to be deemed “complete.” However, this “40 percent” criteria is not included in the federal requirements, and for good reason. The absence of a “completeness” standard in the CMS rules is appropriate as there are countless examples where values will not exist for the five different definitions of standard charge in application to all items, services, and service packages within the hospital’s billing environment. The matrix below illustrates this point:
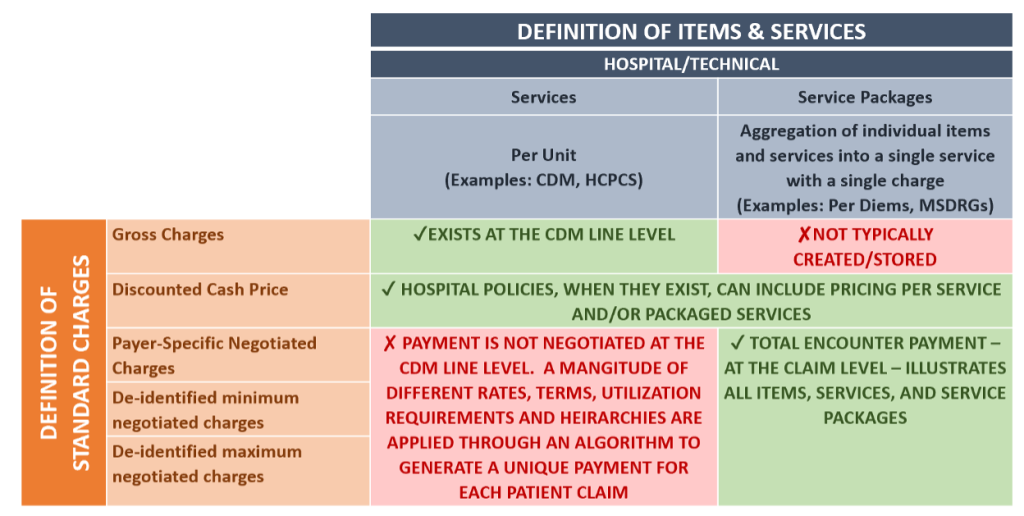
To explain further, standard gross charges are always stored in the hospital’s CDM and are presented at an individual line level with thousands of different lines and prices. Negotiated charges, however, are built on different combinations of these CDM lines to create payment amounts uniquely for each patient claim. These “service packages,” as the rule appropriately describes, cannot be shown on a CDM line-level basis because they do not exist. The converse is also true where payers create payment rates at packaged levels, but the hospital does not store a gross charge. To conclude that both gross charge and negotiated payment amounts will always coincide on a single line is not consistent with the federal requirements and shows a highly uneducated understanding of the hospital billing environment. In sum, it is regrettable that PRA erroneously concludes that a hospital is not providing a “complete” file because it does not report values that simply do not exist.
▪ PRA Finding: 37.2% of the hospitals (744/2,000) did not publish all payer-specific negotiated charges “clearly associated with the names of each third-party payer and plan,” as required.
While CMS requires payers and plans to be identified, some hospitals may not have multiple products by payer. While this is common, it certainly can’t be assumed to exist for ALL payers. The rule requires NEGOTIATED rates to be disclosed. So, if only one Aetna plan has been negotiated, then the hospital would only need to list Aetna once. CMS has provided for a way to indicate this in the new required machine-readable file (MRF) template for July 1, 2024; however, it’s unclear if PRA is not aware that this field is not currently required. What is clear is that PRA seems to be assuming non-compliance based on not finding multiple plan entries for each payer, which would lead to an overstated value of non-compliance.
▪ PRA Finding: 12.0% of the hospitals (972/2,000) did not publish adequate discounted cash prices.
While CMS requires this to be posted if the hospital has developed cash pricing, PRA should not assume that excluding this information means the hospital has determined not to post it. In addition, in the table previously seen, PRA says that it deems a hospital noncompliant for discounted cash price information if the hospital did not provide values for at least 40 percent of the items and services identified. This would appear to be the definition of “adequate.” Still, it is essential that PRA recognize some hospitals do not create discounted cash pricing policies and those that do will not have values for all fields in the file subject to the discussion presented previously.
Separately, PRA also says that it deemed a hospital noncompliant if the hospital’s price estimator tool did not show both the negotiated rates and discounted cash prices. CMS does not require this feature for compliance and, again, does not reflect the fundamental understanding that not all hospitals will have discounted cash prices.
Conclusion
As seen, Patient Rights Advocate is utilizing research criteria to deem hospitals as NONCOMPLIANT that are not present in the federal requirements and are not consistent with industry knowledge. We would have hoped that PRA would have gained a better understanding of these factors in its sixth report, but we clearly see that prior failures persist. We join with AHA and HFMA in calling out this highly inaccurate “research” and ask that PRA conform its criteria to the federal requirements and not its own arbitrary factors.
We believe the organization’s aim to help patients more fully understand anticipated prices for care is a worthy and critical objective and believe more could be done to collaborate to achieve these important goals. As always, we are committed to these same objectives and welcome additional conversation to further the cause.
Have thoughts or questions?
Related