The Impact of Contract Labor on Hospital Costs
Is Contract Labor Impacting Hospital Costs?
The American Hospital Association in March 2023 reported the results of a recent study on contract labor in hospitals.
“Contract labor expenses for hospitals and health systems surged 258% from 2019 to 2022 as nationwide labor shortages forced many to rely on contract staffing firms to meet patient demand, according to an analysis of 2022 data from over 1,000 hospitals and health systems by AHA and Syntellis. Contract labor full-time equivalents jumped 139% over the three-year period, while the median wage rate paid to contract staffing firms rose 57%.” Essentially, organizations had to use more contract labor while also paying exponentially more for the contract labor they used,” the report notes.”
We decided to expand the study by focusing on all acute care hospitals in the US for the period 2019 to 2022 using filed Medicare Cost Reports and to assess the effect of this increase on total hospital expenses per adjusted day. There were three primary questions that we sought to answer:
- Are the initial results of AHA’s study valid when a more complete universe of US hospitals is included?
- Is contract labor usage different across different regions and categories of hospitals?
- Has contract labor usage been a significant factor in increased hospital costs?
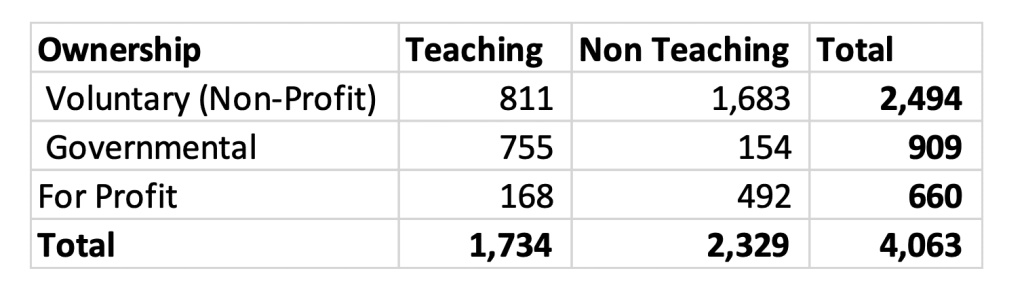
We expanded the study to include 4,063 hospitals that had data for in all 4 years, 2019 to 2022. The composition of our study hospitals is presented below.
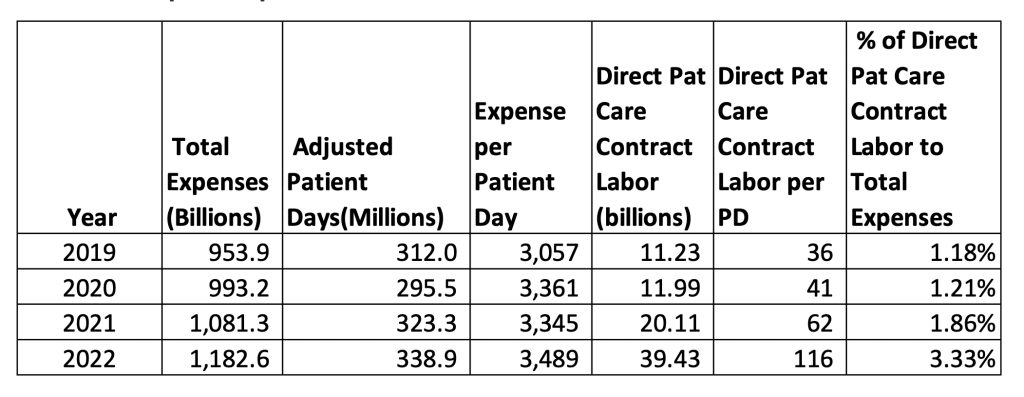
Before focusing on the contribution of contract labor expenses to rising hospital costs, we identified the change in both volume and expenses for the hospital industry. Data in Table 1 shows that total hospital operating expenses for the 4,063 hospitals increased from $953.9 billion in 2019 to $1,182.6 billion in 2022 (a 24% increase) while adjusted patient days increased to 338.9 million in 2022 from 312.0 million in 2019, an 8.6% increase. Because total expenses are increasing at a rate greater than volume, expenses per adjusted day increase to $3,489 in 2022 from $3,057 in 2019, a 14.1% increase. This increase in hospital costs has been cited as one of the primary causes in health insurance costs along with increasing drug costs (Wall Street Journal September 9, 2023).
Table 1: Hospital Expenses and Volumes 2019 to 2022
1. Are the initial results of AHA’s study valid when a more complete universe of US hospitals is included?
Using data from Worksheet S-3 in the Medicare Cost Report and shown in Table 1, we are able to identify contract labor costs associated with direct patient care. In 2019 the total reported value for contract labor associated with direct patient care was $11.23 billion and this value increased to $39.43 billion in 2022, a 251 percent increase. This value is almost identical to the value reported by AHA in their more limited data set. Direct Patient Care Contract Labor (DPCL) expenses accounted for 1.18% of total hospital expenses in 2019 and increased to 3.33% in 2022. The increase in expenses per patient increased by $432 ($3,489 less $3,057) and the increase in DPCL per patient day increased $80 ($116 less $36). While DPCL is a relatively small area of total expense, increases in DPCL accounted for 18.6% of the total increase in hospital expenses. This observation would indicate that DPCL has been a factor in rising hospital expenses.
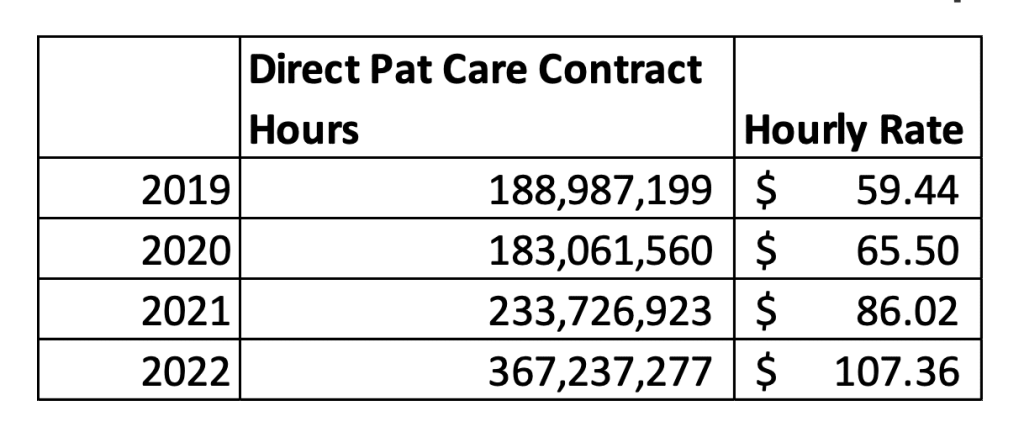
The AHA study also cited a 139% increase in DPCL hours combined with a 57% increase in wage rates. Data from Worksheet S-3 of Medicare Cost Reports shows 2019 DPCL hours were 188.987 million and 367.237 million in 2022 which is a 94% increase and is below the AHA value of 139% (Table 2). Average hourly salary from Worksheet S-3 shows a 2019 hourly wage rate of $59.44 which increased to $107.36 in 2022, an 81% increase which is above AHA’s value of 57%. While our data suggests a similar increase in total DPCL expenses, the data from our larger data set suggests a lower rate of increase in DPCL hours but a larger increase in the average hourly wage rates. This indicates that the employment of contract labor is becoming much more expensive as labor markets tighten.
Table 2: Direct Patient Care Hours and Compensation Rate
2. Is contract labor usage different across different regions and categories of hospitals?
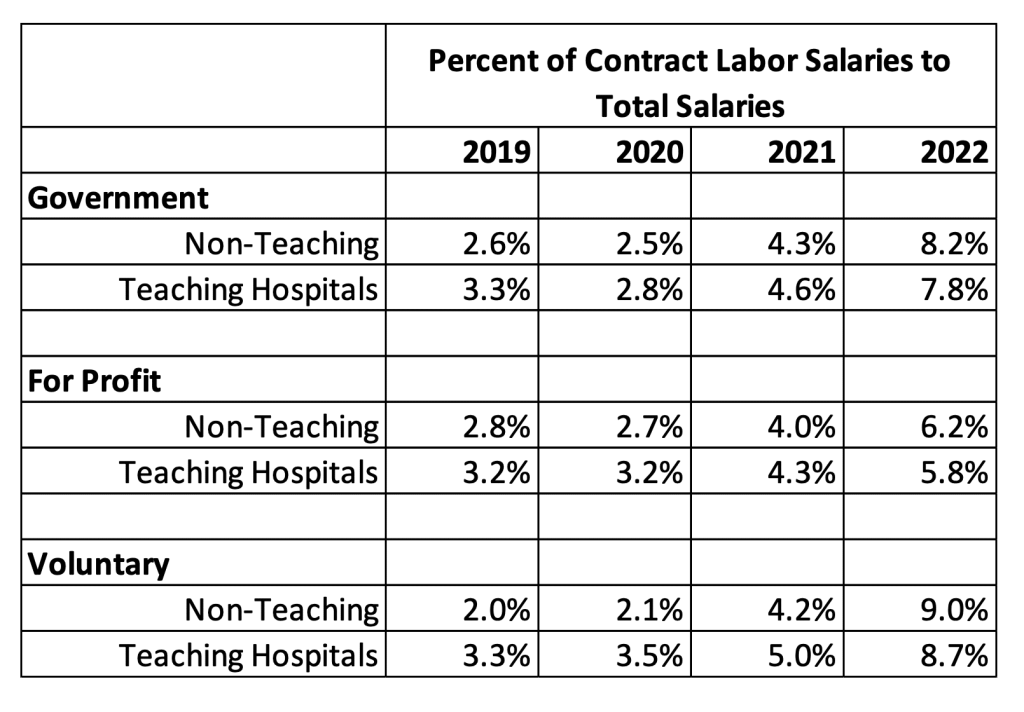
The next component of our analysis was to determine if specific categories of hospitals relied more heavily on contract labor. To do this we looked at the impact of ownership status and teaching designation as well as regional variation. Table 3 shows the percentage of contract labor salaries in direct patient care compared to total salaries. This metric provides a measure of the dependency of the hospital upon contract labor. The data shows three clear trends. First, all hospital categories have shown an increase in the use of contract labor over the study period. Second, For-Profit hospitals are relying less on contract labor than Voluntary and Government hospitals in 2022. This was not true in earlier years and suggests that For-Profit hospitals have managed to control the use of contract labor over time relative to other hospitals. Finally, teaching hospitals were using more contract labor during 2019 to 2021 than non-teaching hospitals across all three ownership categories, but that was reversed in 2022. Teaching hospitals now rely less on contract labor than non-teaching hospitals.
Table 3: Contract Labor Variation by Ownership and Control
The next piece of the analysis was to determine if there were significant variations in the reliance on contract labor by region. We computed the reliance on contract labor as the percentage of DPCL salaries to total hospital salaries for 2022. The results are presented for each state in Table 4. There does not appear to be a discernable regional difference between states with high and low uses of contract labor. New Mexico had the largest use of contract labor while its neighboring state of Utah had the lowest rate.
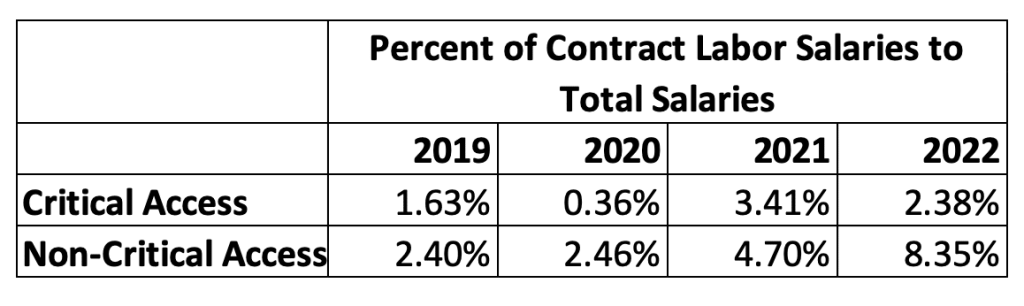
We did notice that hospitals designated as Critical Access used significantly less contract labor relative to non- critical access hospitals in all 4 years See Table 5. The percent of direct patient care contract labor to total salaries was 2.38% in 2022 for critical access hospitals compared to 8.35% for non- critical access hospitals.
Table 4: Contract Labor Variation by State
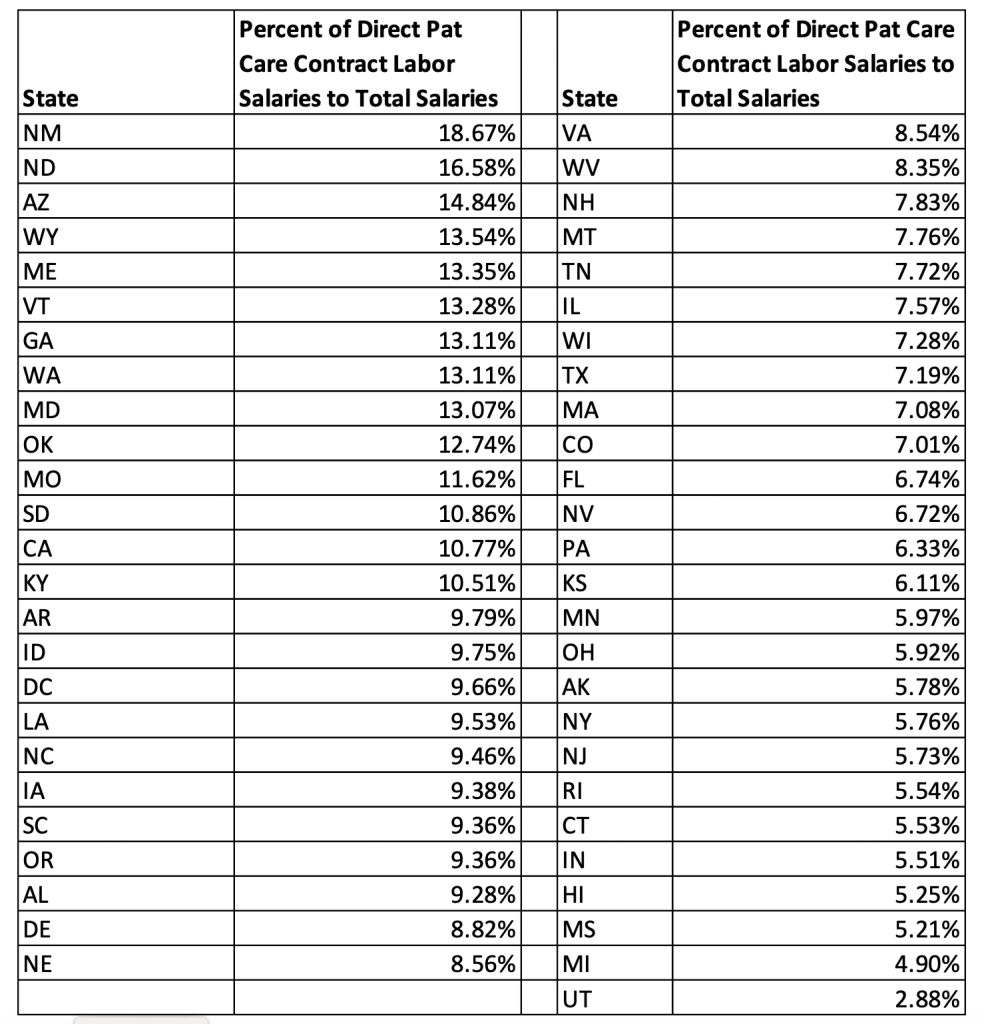
Table 5: Contract Labor Variation by Critical Access Status
3. Has contract labor usage been a significant factor in increased hospital costs?
We have shown earlier that the increasing use of DPCL resulted in higher expenses per adjusted patient day relative to other expense areas. DPCL in 2022 now accounts for 3.3% of total expenses compared to 1.18% in 2019. This however does not necessarily mean that the increasing use of DCPL has led to increasing overall expenses. It is possible that an increasing use of DPCL could help lower expenses in other areas because of improved efficiency. To test this, we ran simple regressions with Expenses per Adjusted Patient Day (EPAPD) adjusted for cost of living against the percent of DPCL salaries to total hospital salaries. We found that there was a statistically significant negative correlation which corroborates our expectation that heavier use of DPCL is associated with higher expenses per adjusted patient day.
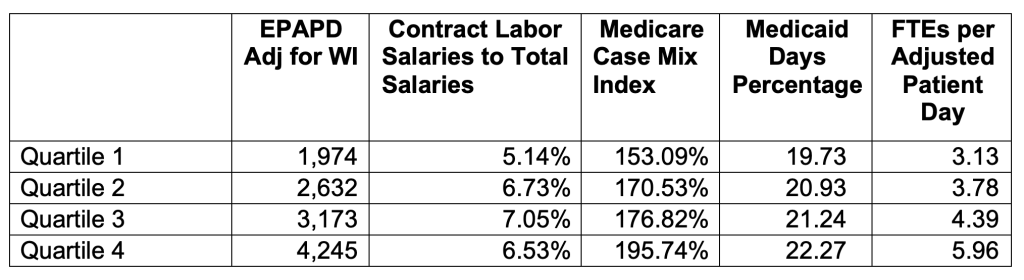
While the relationship between DPCL and EPAPD was statistically significant, other operating factors appeared to have a greater impact on EPAPD. For example, when we ran a regression using DPCL, Medicare Case Mix, Medicaid Days, and FTEs per Adjusted Patient Day against EPAPD, we found that DPCL was no longer statistically significant. This suggests that while DPCL is associated with higher hospital expenses, it is not as important as other variables. Table 6 below shows the relationship of these variables by quartile for EPAPD.
Table 6: Average Values by Quartile for Expense Per Adjusted Patient Day Wage Index Adjusted
Summary
Our review of data from 2019 to 2022 for 4,063 US acute care hospitals documents the use of DPCL has been increasing, and the sharpest increase appears to be in 2022. This corroborates earlier studies that suggested hospitals were still finding it hard to staff key patient care areas, especially nursing, even though Covid is no longer as important as it was in 2020 and 2021. Critical access hospitals are using significantly less DPCL in 2022 relative to other hospitals. This may suggest that these hospitals cannot afford to pay higher salaries for contract labor or an unwillingness of nurses to work in more remote areas. Finally, while DPCL does appear to be a factor in rising hospital expenses, it is not as important when compared to other areas such as case mix complexity, payer mix, and labor productivity.
If you would like more information, we’d love to hear from you! You can contact us here!
Have thoughts or questions?
Related